The Corynebacterium diphtheriae is a gram-positive rod-shaped bacterium belonging to the genus Corynebacteria. It triggers the disease diphtheria.
What is the Corynebacterium Diphtheriae?
The corynebacteria belong to the group of gram-positive rod bacteria. Gram-positive bacteria can be stained blue with the Gram stain. In contrast to the gram-negative bacteria, they only have a thick peptidoglycan layer made of murein and have no additional outer cell wall. Corynebacteria are immobile and cannot form spores. The rod bacteria have the shape of a club due to their swollen cell ends.
They have the ability to grow under both anaerobic and aerobic conditions. The Corynebacterium diphtheriae is 0.5 micrometers in diameter. It is between two and four micrometers long. The grouped arrangement that resembles a V is characteristic of this bacterial strain.
A total of four different biotypes can be distinguished. The gravis, belfanti, mitis and intermedius types differ in terms of sugar fermentation reactions, hemolytic activity and in terms of their colonization formation.
Occurrence, Distribution & Properties
Infections with the Corynebacterium diphtheriae occur worldwide. Most diseases are observed in the temperate climates. Infections are more common in autumn and winter. In the past 50 to 70 years, a sharp decline in infections with Corynebacterium diphtheriae has been observed in the western industrialized countries. However, diphtheria is still endemic in other parts of the world. Endemic areas include Afghanistan, Indonesia, India, Haiti, some African countries and Russia. The last major German epidemic with Corynebacterium diphtheriae was in the years 1942 to 1945. Since 1984 only individual cases of infection have been documented.
For the Corynebacterium diphtheriae, humans are the only relevant reservoir. The transmission occurs when the throat is infected by droplet infection. This transmission variant is also known as face-to-face contact. In skin diphtheria, infection occurs through direct contact. Asymptomatic carriers, so-called eliminators, transmit the pathogen less often than people who are actually sick. Out of 100 people who are exposed to the pathogen, about 10 to 20 fall ill. This corresponds to a contagion index of 0.1 to 0.2.
The contagion index describes the proportion of the non-immune population in which an infection occurs after contact with the respective pathogen causing the disease. Infection through contact with contaminated material is theoretically possible, but rarely occurs. Infections can also occur in the laboratory for occupational reasons. The last reported laboratory infection with Corynebacterium diphtheriae occurred in the 1990s.
The incubation time for an infection with Corynebacterium diphtheriae is two to five days. In rare cases, the first symptoms only appear after eight days. The contagion lasts as long as the pathogen can be detected. Without treatment, most patients are contagious for about two weeks. An infection rarely occurs after more than four weeks. When treated with antibiotics, it is only infected for two to four days.
You can find your medication here
➔ Medication for shortness of breath and lung problemsIllnesses & ailments
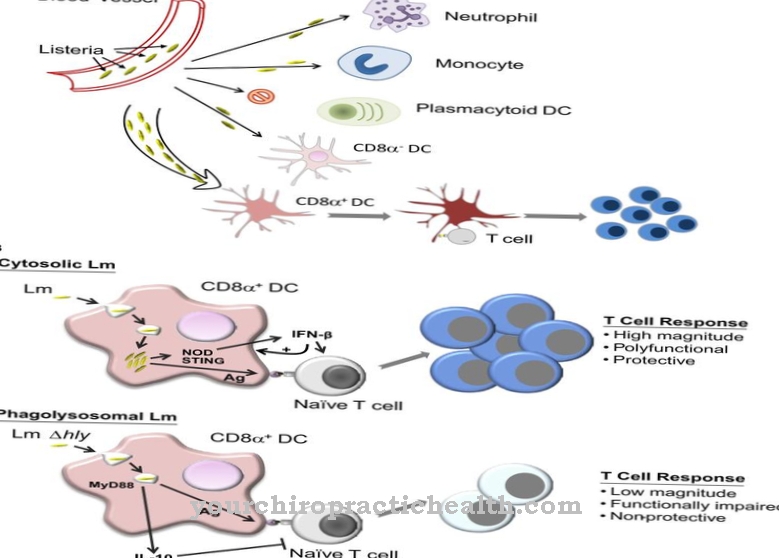
The Corynebacterium diphtheriae can only cause diphtheria if it can produce diphtheria toxins. The exotoxin is only formed when the bacterium is infected by a bacteriophage.Bacteriophages are types of virus that specialize in infecting bacteria.
Infections with Corynebacterium diphtheriae in temperate climates mainly affect the respiratory tract. The primary infection takes place mainly in the area of the tonsils and throat. But there can also be a primary infection of the larynx, nose, windpipe or bronchi.
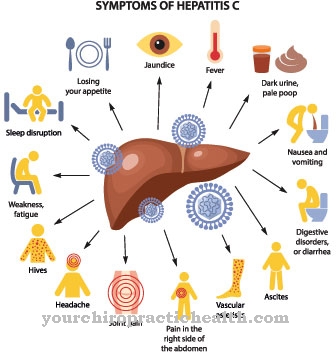
Diphtheria usually begins with a sore throat and difficulty swallowing. The symptoms are accompanied by a fever of up to 39 ° C. Later on, the patients suffer from hoarseness and lymph node swelling. A gray-white coating forms on the tonsils and in the throat. The coating can also appear brownish and is called a pseudomembrane. This pseudomembrane often crosses the tonsils and spreads in the area of the palate and on the uvula.
When trying to lift the membrane with a wooden spatula, punctiform bleeding occurs. This punctiform hemorrhage is an important diagnostic criterion for differentiating diphtheria from other diseases of the respiratory tract. A sweet smell is also typical for diphtheria. It can be perceived from a distance. There is massive swelling in the neck area. They create the characteristic image of the Caesar's neck. The swelling can be so severe that the airways are blocked.
Attacks of suffocation can occur in particular with laryngeal diphtheria, the so-called real croup. Other symptoms of laryngeal diphtheria include cough and hoarseness. Nasal diphtheria is much less noticeable. Often there is only a slightly bloody discharge from one or both nostrils.
The most important complications of diphtheria are attacks of suffocation, inflammation of the heart muscle and inflammation of the nerves. Such polyneuritides can occur weeks after the actual illness. Less common complications are kidney failure, cerebral infarction, encephalitis, or pulmonary embolism.
Skin or wound diphtheria occurs predominantly in tropical areas. In Western countries, risk groups such as the homeless or drug addicts are affected. Based on the clinical picture, a skin infection with Corynebacterium diphtheriae cannot be differentiated from other bacterial skin infections.
Five to ten percent of all diphtheria patients die despite treatment. If treatment is delayed or medical care is inadequate, mortality increases to up to 25 percent.















.jpg)