The Superior Orbital Fissure Syndrome is characterized by the failure of several cranial nerves, which are responsible for supplying various eye muscles as well as the sensitive innervation in the eye area. The clinical picture is very complex and is caused by space-consuming processes.
What is Superior Orbital Fissure Syndrome?

© Sagittaria - stock.adobe.com The superior orbital fissure syndrome is a complex clinical picture due to the failure of several cranial nerves in the area of the superior orbital fissure. The superior orbital fissure is a large space between the small and large sphenoid bone (Sphenoid bone). The middle cranial fossa (Fossa cranii media) with the eye socket (Orbit) connected. The superior orbital fissure serves as an opening for various structures. Underneath are the cranial nerves Oculomotor nerve (Nervus III), Trochlear nerve (IV nerve), Abducens nerve (VI nerve) and a branch of the Trigeminal nerve (V nerve). Of the Trigeminal nerve is a sensitive nerve that is divided into four branches. Only the branch runs from it Ophthalmic nerve (V1 nerve) through this gap.Furthermore, the fissura orbitalis superior is still through the blood vessels Ramus orbitalis arteriae meningeae mediae and Superior ophthalmic vein crosses. Hence the Superior orbital fissure also giving the syndrome its name.
causes
Space-occupying developments in the area of the superior orbital fissure are mostly responsible for the superior orbital fissure syndrome. These can be tumors, aneurysms or thromboses. But inflammatory processes can also impair the function of the corresponding cranial nerves. As a result of tumor growth or other space-occupying processes, nerves III, IV, VI and the branch of nerve V1 can be displaced.
Nervae III, IV, and VI are motor cranial nerves and innervate entire groups of muscles around the eyes. Nervus ophthalmicus (V1) belongs to the sensory nerves and conveys sensory perceptions. In the context of the superior orbital fissure syndrome, all of the nerves running through the superior orbital fissure are often damaged. The oculomotor nerve (Nervus III) innervates four of the six outer eye muscles, two inner eye muscles and the eyelid lifter. Depending on which eye muscles are paralyzed, very complex disorders arise.
In addition to restricted movement of the eyes and a squint, the lifting of the eyelid can also be disturbed and the pupils frozen. The images are seen twice and the close-up does not work. The trochlear nerve (IV nerve) also innervates an external eye muscle. If it is damaged, there is also a squint in combination with double vision. Here the eye deviates inwards and upwards.
If the abducens nerve (VI nerve) is damaged, a so-called inward squint occurs. This nerve is responsible for moving the eye to the side. If the innervation of the lateral rectus muscle is disturbed, the opposing muscle rectus medialis muscle predominates. After all, the ophthalmic nerve (V1 nerve) is responsible for the perceptions in the eye area that are disturbed if it fails.
You can find your medication here
➔ Medicines for visual disturbances and eye problemsSymptoms, ailments & signs
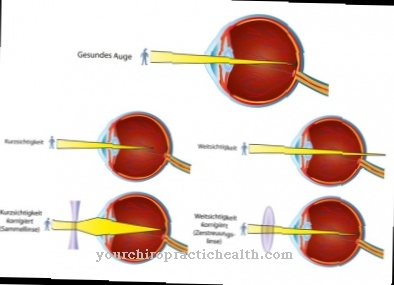
The symptoms of superior orbital fissure syndrome are varied and complex because a whole range of muscles and muscle groups are affected. In addition, the sensitive innervation is also restricted. Massive movement disorders of the eyes occur. In extreme cases, the eye muscles are completely paralyzed (ophthalmoplegia). The eyelid may droop partially or completely (ptosis). The close-up focus is disturbed (accommodation), whereby nearby objects are only perceived as blurred.
In addition, pupillary rigidity often occurs. The pupil no longer reacts to the action of light because the sphincter pupillae muscle is also paralyzed, which is responsible for the constriction of the pupil (miosis) when exposed to light. The occurrence of massive headaches is very typical. Sometimes the eyeball also protrudes due to the space-occupying processes (exophthalmos).
Sometimes there is also a loss of corneal sensitivity. The eyes dry out due to the lack of tears. This creates superficial lesions that lead to even larger defects. Superinfections can develop on these lesions. As a result, creeping and extremely painful corneal ulcers develop.
diagnosis
To diagnose superior orbital fissure syndrome, in addition to strabological examination methods, imaging methods such as magnetic resonance tomography and cranial computed tomography are used. The strabological methods are intended to verify the squint position of the eyes. In the differential diagnosis, the orbital apex syndrome with additional involvement of the optic nerve (nervus II) and the cavernous sinus syndrome must be excluded.
Complications
In most cases, the superior orbital fissure syndrome causes complications and discomfort to the eyes. Since the syndrome is relatively diverse, different restrictions can occur in the individual muscles of the eye area. Most of the time, however, the patient can hardly move his eyes or not at all.
The eyesight is not reduced, but everyday life is made much more difficult because the eyes are no longer mobile. Due to this immobility, those affected by the superior orbital fissure syndrome also suffer from blurred images and can usually only see objects in the vicinity in a blurred manner. As a result, most patients also suffer from dizziness and severe headaches.
This can also lead to sleep disorders and massive restrictions in everyday life. Operating machines or driving vehicles is usually not possible with superior orbital fissure syndrome. Because tearing is also avoided, the eyes often dry out, which can lead to pain. The quality of life is greatly reduced by the superior orbital fissure syndrome.
As a rule, the tumors responsible for the superior orbital fissure syndrome can be removed. This either requires surgery or chemotherapy. The further successes or complications depend heavily on the previous development of the disease. When completely cured, life expectancy will not be reduced.
When should you go to the doctor?
See a doctor as soon as there are problems or changes in the eye area. If there is an inability to move the eye independently, there is cause for concern. A medical examination should be initiated to determine the cause and initiate treatment.
Reduced eyesight, changes in color perception or a dry feeling in the eyes should be clarified by a doctor. If itching occurs due to dry eyes, the risk of open wounds increases. Since germs enter the organism in this way and can trigger further diseases, a doctor should be consulted.
If there is internal pressure in the eye sockets or if there is a headache, a doctor's visit is necessary. If the person concerned suffers from emotional tension in addition to the physical problems, these should be discussed with a doctor. Anxiety, panic or a depressive phase must be treated therapeutically.
If the eyeball protrudes from the eye socket, this is considered unusual. In order not to cause any further illnesses or damage, a doctor should be consulted as soon as possible. If you experience problems with your eyesight under normal lighting conditions, you must see a doctor. In the event of pain, disturbances in sharpness of perception or infections of the eye, a doctor is required to clarify the causes.
Doctors & therapists in your area
Treatment & Therapy
Therapy for superior orbital fissure syndrome can only be successful if the underlying disease is treated. Despite its complexity, the syndrome cannot be viewed as an independent disease. It always represents only one symptom or a complex of symptoms. Further diagnostic examinations must be carried out to verify the cause. Often the last step in tumors is surgery.
This applies equally to benign and malignant tumors. A benign tumor should be operated on if the impairment caused by the space-occupying processes becomes too severe. Malignant tumors and aneurysms pose a deadly threat even without a superior orbital fissure syndrome and should therefore always be surgically removed if possible. For the follow-up treatment of malignant tumors, radiation therapy or chemotherapy or a combination of both is usually necessary. If an operation is no longer possible, symptomatic treatment by administering glucocorticoids can be attempted.
Outlook & forecast
The prognosis of the superior orbital fissure syndrome is tied to the causal disease of the patient. Since the syndrome only occurs as a result of an existing health disorder, the main cause needs to be found and clarified. Tumors, thromboses, or aneurysms can be found to be the cause in most patients.
These damage the cranial nerves and cause problems with vision. In addition, the stage of the underlying disease is decisive for making an overall prognosis. In many cases there are complex impairments that are difficult to treat adequately. In the case of a tumor disease, the time of diagnosis and the location of the tumor, for example, are elementary for the success of the treatment.
If the causal disorder is completely healed, the patient has a good chance that the symptoms of the superior orbital fissure syndrome will improve. However, freedom from symptoms is only possible in rare cases. In most cases, impairments of varying degrees remain, as the activity of the cranial nerves does not always regenerate completely.
In addition, the treatment of the underlying disease is often associated with complications and sequelae. Long-term therapy can be used, or as a follow-up treatment for cancer, therapies are used that trigger further damage to healthy tissue for the purpose of healing in the first step. This must be taken into account when making a forecast.
You can find your medication here
➔ Medicines for visual disturbances and eye problemsprevention
A superior orbital fissure syndrome cannot be prevented because it is caused by processes that occupy space. If benign brain tumors such as meningiomas are present, regular examination for any growth is necessary. If there is a long-term risk that it will displace the nerves, an operation should be considered.
Aftercare
In most cases, the patient with superior orbital fissure syndrome has no special or direct follow-up measures and options. The person concerned is primarily dependent on the diagnosis and treatment of the disease, as this is the only way to prevent further complications and complaints. In general, an early diagnosis with early treatment has a very positive effect on the further course of the superior orbital fissure syndrome.
In most cases with superior orbital fissure syndrome, the person will need to have surgery to remove the tumor. In any case, bed rest should be observed after the procedure so that the person affected can relax and rest. You should definitely refrain from exertion and other stressful activities.
In many cases, patients are also dependent on the support of friends and family in order to cope with everyday life. Since the tumor can spread to other parts of the body due to the superior orbital fissure syndrome, regular examinations should be carried out to prevent this or to detect another tumor at an early stage. In most cases, therefore, the life expectancy of the person affected is also reduced by this disease.
You can do that yourself
Impairments of the eyesight very often trigger a strong fearful experience in those affected. Patients with superior orbital fissure syndrome should therefore acquire various coping strategies in order to experience a good quality of life in everyday life despite the symptoms of the disease. Maintaining the joy of life, optimism and a positive attitude are important in order to be able to meet the challenges in everyday life.
A redesign of the leisure activities should take place so that the sick person can experience a good balance. Relaxation procedures can be used to reduce stress in everyday life. Yoga, meditation or autogenic training are offered in many sports centers and can also be used independently. They strengthen the mental strength and help to achieve an inner balance. To reduce the increased risk of accidents, the patient's surroundings should be adapted to their needs and health conditions.
Self-confidence is to be stabilized by building up a sense of achievement. If the eye problems represent a reduction in wellbeing for the person concerned due to the optical flaw, glasses can be worn to conceal the area. The sick person is well advised if he deals openly with his illness in everyday life. To avoid headaches, periods of rest and sufficient rest are important. Sleep hygiene must be optimized so that a restful sleep is possible.
.jpg)











.jpg)




.jpg)


