At Phosphates is a series of chemical compounds that contain phosphorus. For example, they are contained in adenosine triphosphate (ATP) - the primary energy source in the organism. An increased concentration of phosphate in the blood is possible. a. related to kidney disorders.
What are phosphates?
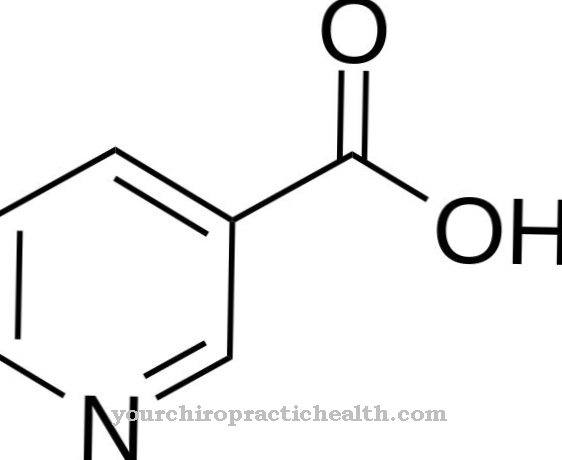
Phosphates are formed from orthophosphoric acid. As salts of orthophosphoric acid, they consist of both positively and negatively charged ions (cations and anions). In contrast, the esters of orthophosphoric acid arise from a chemical reaction of the acid with an alcohol.
Water splits off in the process. Both salts and esters of orthophosphoric acid occur in the organism only in oxidized form. The compounds are only sparingly soluble in water. Phosphates can be divided into three groups. The primary or dihydrogen phosphates have two hydrogen atoms. In contrast, the secondary phosphates or hydrogen phosphates have only one hydrogen atom per phosphate compound. The tertiary phosphates manage entirely without a hydrogen atom.
However, these three variants are not the only possible subdivisions. In addition, phosphates can be present as condensates. These arise by splitting off water. At the end of the biochemical reaction, diphosphoric acid is formed, which owes its name to the two phosphor particles.
Function, effect & tasks
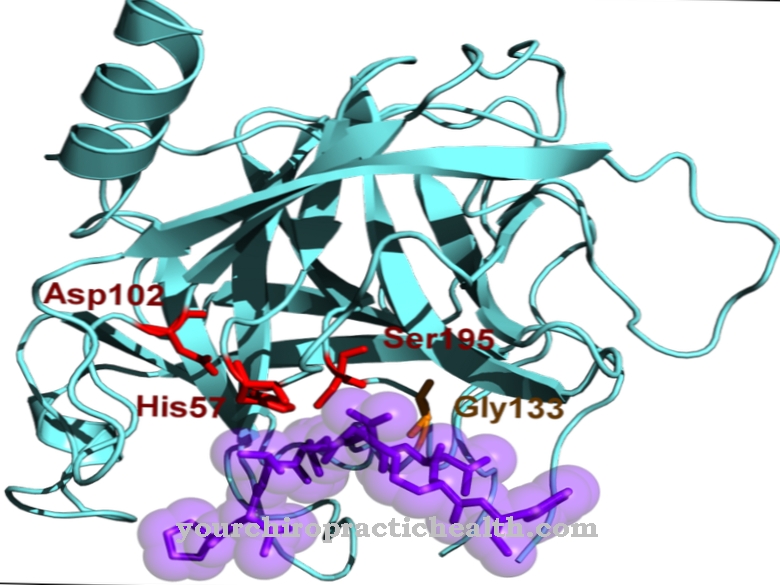
Phosphates are vital for the human body - but all other living things are also dependent on the chemical compound. As an ester of phosphoric acid, it forms part of the nucleic acids. Deoxyribonucleic acid, or DNA for short, consists of the nucleic acids; it stores all hereditary information and controls the metabolism of the cells.
Human DNA consists of the four nucleic acids adenine, thymine, guanine and cytosine, whereby adenine and thymine as well as guanine and cytosine can form a so-called base pair. A long chain made up of the various nucleic acids forms a specific code that the cells translate into protein chains and thus read out. These protein chains can represent messenger substances or building blocks for microscopic cell structures. In addition, phosphates play a key role in the energy metabolism.
As adenosine triphosphate (ATP), they form the primary energy source within the organism. ATP consists of three phosphates, a sugar molecule (ribose) and an adenine residue. The splitting off of a phosphate releases chemically bound energy. What remains is a compound that consists of two phosphates: adenosine diphosphate. Cells use the released energy for almost all processes. The muscles are also dependent on ATP. Its fibers consist of fine filaments that push into one another when they contract, thereby shortening the muscle.
ATP has a softening effect in this process: It loosens the fine fibers from one another and thereby allows them to move again. Rigor mortis is a result of the lack of ATP.
Education, occurrence, properties & optimal values
The optimal value for the phosphate in the blood is 0.84–1.45 mmol / l. This area represents the general frame of reference. These comparison values may not be applicable: Depending on the test used, the examining laboratory may issue other reference values that are then valid. On average, a person consumes around 1000–1200 mg of phosphate.
However, the digestive system does not absorb the full amount, only around 800 mg. The intracellular space stores most of the phosphates that come from food. As an intracellular space, biology summarizes all spaces in cells. However, the cells do not metabolize the phosphates directly, but initially only absorb them. The intracellular space holds 70% of the phosphates. Another 29% is in the bone. The phosphates are stored in the so-called mineralization front, where they are available to the body for further use and thus do not become a permanent part of the bone.
The remaining 1% of phosphates circulate in the blood. Medicine summarizes the phosphate stores in the intracellular space, in the bones and in the blood as a phosphate pool. The phosphate pool is the totality of phosphates in the body that are exchangeable. The bones can also bind calcium phosphate permanently; they only give it up again in severe deficiencies, which can lead to osteoporosis (bone loss).
Diseases & Disorders
An unusually high level of phosphate manifests itself clinically as hyperphosphatemia. A blood test can confirm the findings. Hyperphosphatemia can have various causes. In addition to an unusually high intake of phosphates through food, kidney failure, kidney disorders and tissue destruction are possible triggers.
The kidneys play an important role in regulating the amount of phosphate in the body. They filter the urinary substances, which also include phosphates, from the blood and excrete them in the urine. In this way you can regulate an intake of up to 4000 mg / d. Higher amounts can trigger hyperphosphataemia. In acute hyperphosphataemia, the phosphate level rises sharply.In this case, the disease manifests itself in symptoms such as diarrhea, nausea, vomiting, loss of appetite, muscle cramps, cardiac arrhythmias, seizures and circulatory collapse. There is also a risk of sudden cardiac death.
Secondary hypocalcaemia may develop in which the calcium level in the blood falls below 2.2 mmol / l. Possible symptoms are paresthesia and paws in the arms. Hypocalcemia is based on the fact that calcium is precipitated in the tissue during acute hyperphosphataemia and is therefore no longer bound in the blood.
Chronic hyperphosphatemia can originate from kidney failure. In this case, the organs are no longer able to regulate the amount of phosphate in the blood. Often other consequences of kidney failure occur besides chronic hyperphosphataemia. It increases the risk of heart attacks, strokes and blocked blood vessels. Dialysis treatment is an option for therapy.