Of the atrioventricular septal defect is a congenital heart defect. It is a combination of atrial septal defect and ventricular septal defect.
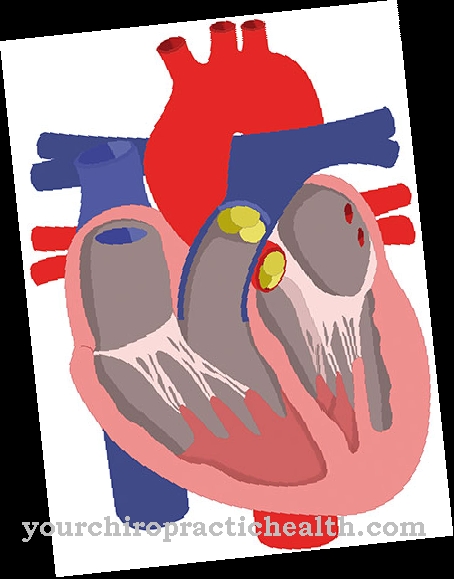
What is an atrioventricular septal defect?

© bilderzwerg - stock.adobe.com
The atrioventricular septal defect is a congenital heart malformation and one of the most complex congenital heart defects. Since the combination of atrial septal defect and ventricular septal defect creates a connection (shunt), the heart defect is one of the so-called shuntvitia. Shuntvitia are congenital heart defects in which the arterial and venous limbs of the bloodstream are connected to one another.
In the case of atrioventricular septal defect, a double left-right shunt forms. The defect is divided into three categories depending on its severity:
- complete atrioventricular septal defect
- partial atrioventricular septal defect
- Ostium primum defect.
In 35 percent of the cases, there are other accompanying heart defects or anomalies of organs.
causes
The exact cause of the malformation is unknown. Every year around 0.19 per 1000 newborns are affected. Girls and boys get sick about the same frequency. The error occurs very often in connection with Down's syndrome. Around 43 percent of all patients with an atrioventricular septal defect also have Down syndrome.
Children are born with a large defect in the heart septum. There is a hole in both the atrial septum (artrial septal defect) and in the septum of the chambers (ventricular septal defect). The heart valve between the left atrium and left ventricle (tricuspid valve) and the valve between the left ventricle and left atrium (mitral valve) are malformed. In addition, the aortic valve is shifted forward and upward. The aortic valve lies between the left ventricle and the aorta.
Symptoms, ailments & signs
Whether and which symptoms appear in the newborn depends on the size and location of the defect. The strength of the blood flow, the pressure level in the lungs and the extent of the valve defects also influence the symptoms of the heart defect. The anomalies do not play a role before the birth, as the child is supplied with oxygen-rich blood from the mother. After birth, oxygen is no longer absorbed through the mother, but through the child's lungs.
To do this, the lungs have to unfold and the pulmonary vessels expand. In the case of a large atrioventricular defect, the high pressure that prevails in the left heart pushes the blood through the wall defect into the right half of the heart. This medical phenomenon is known as a left-right shunt. In the right heart, the extra blood increases the pressure. The blood flows through the pulmonary vessels at increased pressure and thus stresses the lungs.
Both heart chambers also have to do a lot more work. The right half of the heart suffers from the increased pressure, the left half is affected by the increased blood flow from the lungs. Because the AV valve is unable to close, further blood flows back into the left heart. This must also be ejected with each heartbeat. Even within the first few days of life, the child's heart is so stressed that it leads to heart failure.
The affected children suffer from shortness of breath and show water retention all over their bodies. The skin, eyelids, and liver are swollen. The children become increasingly weak and refuse to drink. In some cases, there is a pressure reversal through a protective mechanism.
In this case, oxygen-poor blood from the right heart passes through the septal defect into the left heart. Here the lips and the mouth region are colored blue. If the high blood pressure is fixed in the lungs, surgery can no longer be performed. Children with such fixed pulmonary hypertension have a maximum life expectancy of 10 to 20 years. Usually, however, the artrioventricular septal defect is detected early.
Diagnosis & course
A heart murmur can be heard with the stethoscope during auscultation in the first week. This is caused by the backflow of blood through the defective AV valve. An electrocardiogram can be performed if an atrioventricular septal defect is suspected. This provides specific information about the heart defect. The X-ray shows a significantly enlarged heart.
The gold standard for fully assessing the severity of the heart defect is echocardiography. If an atrioventricular septal defect is suspected during pregnancy, a prenatal risk assessment can be performed. From the 16th to 20th week of pregnancy, a heart defect can be diagnosed with certainty with this method.
However, the heart defect cannot be detected with normal routine ultrasound examinations. The examinations take place in specially trained perinatal centers.
Complications
In the case of a fully developed atrioventricular septal defect (AVSD), all four heart chambers are connected to one another from birth due to a heart malformation.This means that arterial and venous blood are constantly mixed and the efficiency of the heart's pumping capacity is greatly reduced.
Complications that arise as a result of the untreated AVSD are usually high pulmonary pressure (pulmonary hypertension), which, as a physiological counter-reaction, leads to a thickening of the muscular middle wall (media) of the pulmonary arteries. In a kind of vicious circle, the two effects reinforce each other (Eisenmenger reaction). The increasing insufficiency of the heart leads to a poor prognosis if left untreated.
Open-heart surgery can very well improve the long-term prognosis. The most important steps during the operation are the reconstruction of the two atrioventricular heart valves, the mitral valve in the left and the tricuspid valve in the right heart, and the removal of the septal defects by applying artificial patches. In addition to the classic surgical risks associated with open heart surgery on a baby or toddler, there is a specific risk in a disruption of the electrical excitation system.
The AV node, which collects the electrical impulses from the clock (sinus node) and transmits them to the downstream systems with a slight delay, is usually particularly affected. If the problem cannot be solved with medication, an artificial pacemaker must be implanted.
When should you go to the doctor?
A genetically determined atrioventricular septal defect (AVSD) becomes symptomatic in the newborn within the first few days. There is no need to ask when medical help must be sought. The severity of the heart malformation can be determined by means of echocardiography and confirmed and supplemented by ECG findings. With a fully developed AVSD, all four heart chambers are connected to one another and, if left untreated, the prognosis for the newborn is extremely unfavorable.
During a surgical procedure in a special clinic, the connections between the two chambers are closed and the two inoperative heart valves between the left atrium and left chamber (mitral valve) and between the right atrium and right chamber (tricuspid valve) are usually replaced. Such an intervention improves the survival prognosis for the newborns dramatically.
For those affected, an almost normal life is usually possible after a successful operation if the reconstructive operation is carried out early enough and no irreversible damage to the lungs or heart muscle has yet formed.
After reaching adulthood, the intervals for medical check-ups can be extended if the symptoms remain free. However, those affected should watch out for specific symptoms that could indicate a new problem and that must be clarified immediately by a cardiologist or an experienced family doctor.
Doctors & therapists in your area
Treatment & Therapy
If the heart defect is not treated, only 10 percent of the affected children are still alive after six months. The patients develop pulmonary hypertension and as a result a so-called Eisenmenger reaction. Most atrioventricular septal defects are discovered early and are operable.
Using the heart-lung machine, the arterial and venous circulation are separated from each other again. In the first six months after the operation, medical endocarditis prophylaxis is carried out in accordance with current medical guidelines. Regular check-ups must also be carried out after the operation. The long-term prognosis of the operated children is very good. A second operation is rarely required.
Outlook & forecast
The prognosis of an atrioventricular septal defect is poor. If healing takes place, there is an increased risk of suffering a secondary disease. Over 35% of patients develop other heart diseases that are lifelong and no longer curable. Down syndrome is diagnosed as the underlying disease in the majority of patients. About ¼ of those with atrioventricular septal defect are among them.
The diagnosis and the start of treatment are essential for the prognosis. The children are born with the defect and need therapy as soon as possible. Without medical care, there is a risk of premature death within the first few weeks or months of life.
Statistics show that untreated children have an approximately 90% chance of dying within the first 6 months of life. The shortness of breath and non-functional heart activity put such a strain on the organism that there are hardly any chances of survival without intensive medical therapy. Multiple organ failure or death from suffocation would be the devastating consequences.
In professional medical care, the heart's activity is stabilized with a heart-lung machine. This improves the prospect of survival considerably. As soon as the child is in a stable state of health, an operation is carried out. This significantly increases the probability of survival and enables the patient to have sufficient independent cardiac activity.
prevention
Since the exact causes of the atrioventricular septal defect are unknown, the disease cannot be prevented. If a child with the heart defect has already been born in a family, there is a risk of recurrence of 2.5 percent if another child is born. Especially in families with such an increased risk of the disease, prenatal diagnostics can help to identify the heart defect at an early stage. The earlier the diagnosis is made, the better the prognosis.
Aftercare
With this disease, in most cases there are no or only very few options and measures available for follow-up care. The person concerned is first of all dependent on a comprehensive and, above all, early diagnosis in order to permanently alleviate the symptoms and to recognize the heart defect at an early stage. Since this is also a congenital disease, it cannot be treated causally, but only purely symptomatically.
Complete healing cannot occur, and self-healing cannot occur either. In most cases, this defect is relieved by surgery. The further course depends very much on the time of diagnosis, so that no general prediction can be made. After such an operation, the person concerned should definitely rest and take care of his body.
You should refrain from strenuous or stressful activities in order to avoid unnecessary stress on the heart. Regular checks and examinations are also necessary after the procedure. If the procedure is successful, there will be no reduced life expectancy for those affected. However, most people also have other heart problems that also need treatment.
You can do that yourself
The atrioventricular septal defect as a congenital heart disease represents a daily challenge for affected families. Prenatal diagnostics are indispensable in order to detect the heart defect at an early stage, especially when the risk of the disease is increased. However, it is often possible for those affected to lead an almost normal life.
However, regular intervals for medical follow-up checks and strict adherence to medication plans are advisable. Other important aspects are avoiding nicotine and leading a healthy lifestyle. To avoid psychogenic stress, emotional stress and social law issues, it is advisable to consult self-help groups and suitable therapists. Problems such as: special educational needs, sporting restrictions, school disadvantage compensation or relaxation procedures can be clarified.
Mental and physical agility promote self-confidence and have stabilizing properties. Those affected are therefore encouraged to take an active part in public life on their own initiative. Exercising hobbies here serves as a sensible introduction and motivational aid. Well-organized trips and excursions make a significant contribution to a healthy quality of life; renouncing it has a negative effect on the mental state.
The support of family and friends as a strong social network can also increase one's own well-being and reduce tension. Further information on the subject of heart disease is also available from the Deutsche Herzstiftung e.V. and the Federal Association of Children with Heart Disease.






.jpg)


.jpg)





.jpg)
