Of the Scalenus anterior muscle Together with a total of three paired scalene muscles, it belongs to the deep neck muscles. It arises from cervical vertebrae 3 to 6 (C3-C6) and extends diagonally to the 1st rib. The anterior scalenus muscle fulfills three main mechanical tasks: it is involved in the lateral flexion and rotation of the neck and, in its function as an auxiliary breathing muscle, in the elevation of the 1st rib.
What is anterior scalene muscle?
The anterior scalene muscle, like the other two scalene muscles, is paired and belongs to the deep neck muscles. The German designation "anterior rib holder muscle" indicates its function as an auxiliary respiratory muscle.
The muscle arises from the cervical vertebrae C3 to C6 and pulls obliquely sideways to the 1st rib, so that when the cervical spine is contracted and fixed on both sides, a pull is exerted on the first rib, so that the rib and thus the thorax rise. This means that the process of inhaling is supported. Between the anterior scalenus muscle and the medius scalenus muscle, i.e. between the anterior and middle rib support muscles, there is a triangular gap, the scalenus gap, through which nerves and blood vessels run. Among other things, the subclavian artery runs through the scalene gap.
It is an important, paired body artery, of which the left branch arises directly from the aortic arch and the right branch from the trunk common to the right cervical artery (Truncus brachiocephalicus). branches off. The two arteries supply the head, neck, shoulders and arms with oxygenated blood. The nerves running through the scalene gap originate from the brachial plexus, the plexus of nerves whose branches innervate the arms, shoulders and chest.
Anatomy & structure
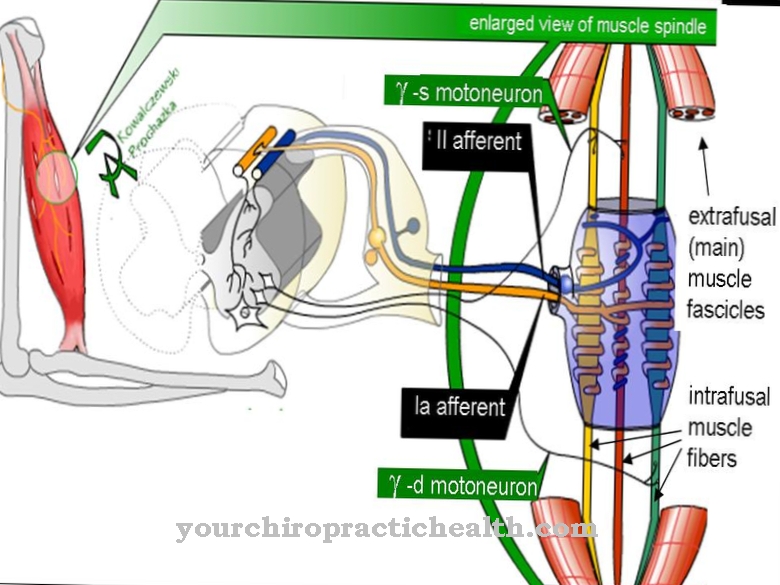
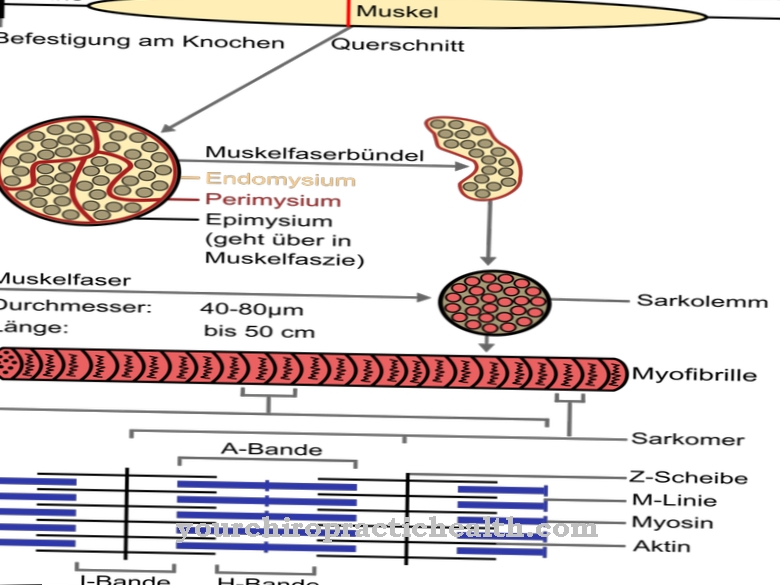
The anterior scalenus muscle, the anterior rib support muscle, corresponds in anatomical structure to the skeletal muscles. Its muscle tissue consists mainly of striated, red muscles, which have a high proportion of myoglobin because the muscle is often exposed to constant stress.
The skeletal muscles are characterized by the fact that the force exerted during the contraction of the muscle fibers can be continuously dosed by means of appropriate nerve impulses. Another characteristic feature is that the tension of the skeletal muscles is largely subject to voluntary control. In order to fulfill its main function, the lifting of the first rib or the entire thorax, the anterior scalene muscle needs a good counter bearing. It therefore fans out at the upper end, so that when it contracts, the unilateral tensile load is divided between the four cervical vertebrae C3 to C6 and the problem of a herniated disc in the cervical area is minimized.
At the lower end, the two rib holding muscles are attached to small bumps (tubercula) specially designed for this purpose on the first costal arch (tuberculum musculus scalene anterior). The sensory and motor innervation takes place through spinal nerve branches that emerge from the spinal canal between the cervical vertebrae C5 to C7.
Function & tasks
One of the main tasks of the two anterior scalene muscles is to actively support breathing. Simultaneous contraction of the two anterior rib holding muscles pulls the ribs upwards. This expands the chest cavity so that inhalation is supported. In other functions, the two muscles significantly support a lateral flexion of the neck and a lateral rotation in the horizontal plane.
Neck flexions to the right or left and head rotations to the right or left can be achieved by unilateral contraction of the right or left anterior scalene muscle. In addition to the motor tasks, the two anterior rib support muscles also have a protective function. The inclined course from the first costal arch to the cervical vertebrae creates a triangular space to the scalenus medius muscle, the scalenus gap. It serves to pass through and protect important blood and nerve vessels that supply the head, shoulders and arms with oxygen-rich blood or innervate them in terms of sensory and motor functions.
You can find your medication here
➔ Medicines for back painDiseases
Chronic stressful situations or other causes that lead to a hardening of the anterior or middle rib support muscle can narrow the scalenus gap, so that pressure is exerted on the subclavian artery or on the nerve fibers of the brachial plexus (nerve compression).
The narrowing of the scalenus gap leads to the so-called scalene syndrome, which can manifest itself as pain in the forearm or paresthesia in the hand. Symptoms such as tingling, numbness and coldness are typical companions of a scalene syndrome. If the subclavian artery is also compressed, the result is an inadequate blood supply and, in many cases, even a drop in blood pressure. Similar symptoms are caused by "thoracic outlet syndrome," also known as shoulder girdle compression syndrome, in which nerve fibers, the main artery and the main vein (subclavian vein) are all affected by compression.
One possible reason for the bottleneck is an enlargement (hypertrophy) of the anterior scalene muscle. Excessive contraction of the anterior rib support muscle can cause hyperadduction syndrome, which manifests itself as excessive upward movement of the uppermost rib to which the muscle is attached. In the course of this, the nerves are also compressed with symptoms comparable to those described above. The symptoms usually occur at night, with women being more often affected than men.
The fact that nerve compression in the neck area leads to paresthesia and symptoms of paralysis in the arms and shoulders is what modern anesthesia makes use of in surgical interventions in the shoulder area and arms. In a regional anesthetic procedure, the brachial plexus is numbed in the scalenus gap. There is no need for general anesthesia.





















.jpg)



