The Pediatric audiology deals with children's hearing, voice, swallowing and speaking disorders as well as disorders in language development. Together with phoniatrics, pediatric audiology forms an independent specialist area, which was managed as a sub-area of ear, nose and throat medicine (ENT) until 1993.
Both pediatric audiology and phoniatrics have a strongly interdisciplinary character because the problems that arise are often not of purely organic origin, while pediatric audiology provides cross-disciplinary diagnoses and therapies regardless of this.
What is pediatric audiology?

Central topics in diagnosis and therapy in pediatric audiology are voice, speech and language development disorders in children as well as hearing and perception disorders. Swallowing disorders in children also fall into the treatment and diagnostic spectrum of pediatric audiology, because the issues are often causally related. Pediatric audiology often pursues interdisciplinary, holistic approaches in its diagnostic and therapeutic procedures beyond the examination and treatment of organic abnormalities.
There are interlinkings with the medical fields of ENT, orthodontics, neurology and psychiatry and with non-medical fields such as psychology, speech therapy, phonetics, pediatrics and many others. Together with phoniatrics, pediatric audiology forms an independent specialist area. The original name was specialist in phoniatrics and pediatric audiology. As of January 2004, the new name will be specialist in speech, voice and children's hearing disorders. The additional specialist medical training lasts a total of 5 years and includes specialist training in child development disorders with regard to hearing, voice, speaking, speech and swallowing.
The interdisciplinary character of this medical specialty was the first Hermann Gutzmann sen. 1905 in his habilitation thesis. Pediatric audiology in particular received a further boost in 2009 with the introduction of newborn hearing screening. Babies who are suspicious of hearing screening are referred to pediatric audiology for further treatment.
Treatments & therapies
One of the main concerns of pediatric audiology is to identify causes of childhood developmental disorders in the area of hearing perception and in voice and language development in order to apply targeted therapies in a mostly holistic and interdisciplinary approach. The subject area also includes the act of swallowing, which is closely linked to voice and language development and therefore falls within the diagnostic and treatment spectrum of pediatric audiology.
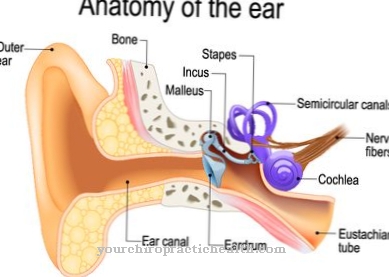
Since January 2009, audiometric newborn screenings have been carried out as standard, in which congenital, i.e. primarily genetic, hearing disorders are detected so that they can be recognized and treated at an early stage. In the hearing screening, only methods that allow an objective measurement are considered. Hearing disorders can have many causes; the entire spectrum of hearing disorders ranges from clogging of the external auditory canal with wax plugs or foreign bodies to sound conduction problems in the middle ear and sensorineural disorders.
While sound conduction problems can mostly be traced back to organic-physical reasons, sound sensation disorders are problems with the conversion of sound waves into electrical nerve impulses in the cochlea in the inner ear or functional impairments of the auditory nerve (vestibulocochlear nerve) due to lesions or disease or around Problems in the brain in processing the nervous hearing impulses. Detected anomalies in children's speech development can arise due to impaired hearing performance, but are often based on other causes such as voice disorders, which can also be of organic origin, or on speech and flow disorders such as stuttering, articulation disorders (dyslalia) or on a variety of acquired or inherited Voice disorders.
An example of an absolutely necessary interdisciplinary approach with regard to diagnostics and therapy is selective or total mutism, the partial or total loss of language after having fully learned the language although no direct organic causes for the no longer speaking are recognizable. Functional or neurogenic swallowing disorders or swallowing disorders after certain surgical interventions also often interact with voice and language development.
You can find your medication here
➔ Medicines to improve concentration and language skillsDiagnosis & examination methods
The spectrum of possible developmental disorders that lead to acquired or inherited organic anomalies or to interdisciplinary problems with the further processing of sensory impressions and the development of language skills is very broad and varied. The corresponding range of diagnostic methods is just as diverse, in order to develop efficient and targeted therapies based on them. In the hearing screening for newborns, which has been planned since January 2009, mainly brain stem audiometry and / or methods using otoacoustic emissions are used.
With the brain stem method BERA (brain stem evoked response audiometry), slight acoustic stimuli are applied to the newborn's ear and the brain waves are measured using a few electrodes. They allow conclusions to be drawn about the function of the auditory nerve and the processing centers in the brain. The test, which takes about 20 minutes, is carried out during the baby's normal sleep and does not bother the child. The other method - called TEOAE (transitory otoacoustic emissions) - makes use of the fact that the outer hair cells in the cochlea respond to sound stimuli like an amplifier with their own sound stimuli that are measurable. A tiny probe containing a loudspeaker and microphone is inserted into the external ear canal for examination.
So-called clicks are generated with the loudspeaker and the sound waves that the outer hair cells generate a few milliseconds later are measured with the loudspeaker. Both methods are largely automated, but have the disadvantage that recognized abnormalities are not always based on problems with the further processing of sound stimuli or on problems with the conversion of mechanical sound stimuli into electrical nerve impulses. Positive diagnoses therefore require careful further clarification through further diagnostic procedures.
A large number of objective and subjective audiometric methods are available for measuring hearing impairment in children from around 3 years of age and older. Hearing problems can also arise as side effects of certain antibiotics and diuretics (water tablets).In the case of swallowing disorders, the fiber endoscopic swallowing examination (FEES) has established itself as an imaging diagnostic method, in which the nose and throat can be inspected via an optical fiber. In some cases the FEES has to be supplemented by a video-supported VFS.









.jpg)


.jpg)





.jpg)
