The Substantia nigra represents a core area in the midbrain that is darkly colored and belongs to the extrapyramidal motor system. It thus contributes to the control of movements. A decline of the substantia nigra occurs in Parkinson's syndromes and leads to the development of the cardinal symptoms rigor, tremor, bradykinesia and postural instability.
What is the substantia nigra?
The substantia nigra is located symmetrically in both halves of the brain (hemispheres) and belongs to the midbrain. There it borders on the cerebral crura (crura cerebri) and the midbrain hood (tegmentum mesencephali). The name of the substantia nigra goes back to its black color, which is based on the high amount of melanin and iron in this area.
Dopamine functions as the most important neurotransmitter in the substantia nigra, occurs as a messenger substance only in the central nervous system and belongs to the group of biogenic amines. These are neurotransmitters that arise from the amino acid tyrosine and lose a carbon dioxide molecule through decarboxylation. In addition to dopamine, the biogenic amines also include serotonin, adrenaline and noradrenaline.
Anatomy & structure
Anatomically, the substantia nigra can be divided into two areas: the pars compacta, also known as the zona compacta, and the pars reticulata. The pars compacta consists of closely arranged nerve cells that contain a large amount of the pigment melanin. Nerve fibers connect the pars compacta with the striatum.
In addition, the pars compacta belongs to the black system (nigrostriatal loop). This also includes the ruber nucleus, which is also located in the midbrain, and nuclei of the striatum. Compared to the nerve cells of the pars compacta, the neurons of the pars reticulata are less close together and contain a lot of iron, which gives the tissue a reddish color. This area also includes the pars lateralis, which some experts consider to be an independent part. The pars reticulata of the substantia nigra has connections to the striatum and the ventrolateral thalamus. Other nerve fibers lead from the substantia nigra to the cerebral cortex and the subthalamic nucleus.
Function & tasks
The substantia nigra belongs to the extrapyramidal motor system and is therefore involved in the control of movements. In this context, it has a starter function, as it is particularly involved in initiating movement and planning.
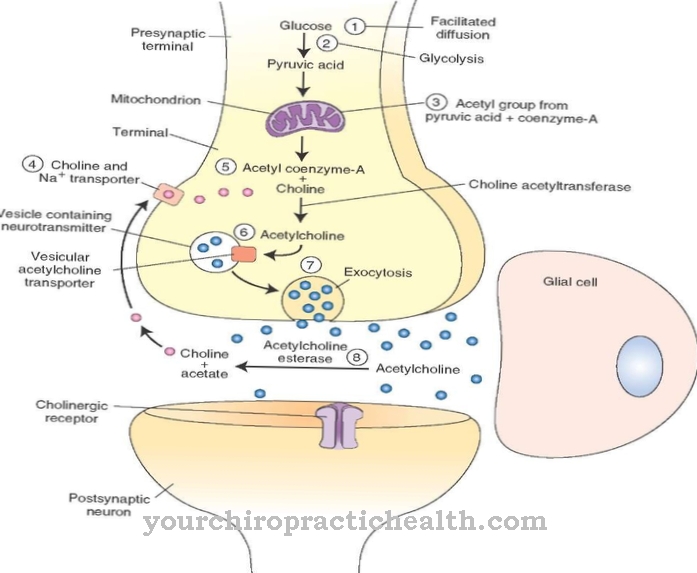
The extrapyramidal motor system also includes the basal ganglia, the motor cortex and various core areas in the brain, including the ruber nucleus in the midbrain and the reticular formation, which runs through the hindbrain, midbrain and diencephalon. Like the substantia nigra, all of these structures are dependent on dopamine as a neurotransmitter: nerve cells form the messenger substance in their terminal knobs and store it in vesicles. If an electrical impulse - a so-called action potential - reaches the end of the nerve fiber and thus the end knobs, the cell releases the dopamine into the synaptic gap.
The messenger substance crosses the gap between the presynaptic and postsynaptic nerve cells and attaches to receptors in the postsynaptic membrane, whereupon ion channels open in it. Charged sodium particles can flow into the cell through the channels and change the electrical charge of the neuron. If the change exceeds the threshold potential, a new action potential arises in the postsynaptic nerve cell. Dopamine deficiency leads to a disruption in this process and thereby impairs human motor skills. As a whole, the extrapyramidal motor system is primarily responsible for gross motor movements.
You can find your medication here
➔ Medicines to calm down and strengthen nervesDiseases
Parkinson's disease is associated with a decline in the substantia nigra, which leads to the development of the characteristic symptoms of the disease. Parkinson's syndrome is a neurodegenerative disease and is also known as paralysis.
In 1917, James Parkinson was the first to describe the syndrome; Today around 250,000 people in Germany suffer from the disease, three quarters of which are due to the idiopathic Parkinson's syndrome. The cardinal symptoms are rigor, tremor, bradykinesia / akinesia, and postural instability. Rigor is muscle rigidity or stiffness that arises due to increased resting tone: the affected muscles are excessively tense. On the other hand, the second main symptom, tremor, manifests itself as muscle tremors and primarily affects fine motor movements.
In addition, those affected typically suffer from slowed movements; medicine calls this phenomenon bradykinesia. While patients with bradykinesia can in principle perform movements - albeit at a slower rate - with akinesia they are only partially able to do so (lack of movement) or not at all (immobility). The postural instability leads to an unsafe posture and, as a result, often to a slightly bent gait. The combination of bradykinesia with rigidity, tremor and / or postural instability often leads to gait disorders and other functional impairments.
In addition to idiopathic Parkinson’s syndrome, medicine distinguishes three other forms. Familial Parkinson's Syndrome is due to defects in the genetic make-up - various genes can be considered as the cause. In contrast, symptomatic or secondary Parkinson's syndrome develops as a result of another underlying disease such as Binswanger's disease or Wilson's disease, or due to medication, drugs, poisoning, or injury. The fourth form of Parkinson's syndrome is also a consequence of other diseases; However, these are specifically neurodegenerative diseases that manifest themselves in the loss of nerve cells.
These include Lewy body dementia, multiple system atrophy, progressive supranuclear palsy, and corticobasal degeneration. L-dopa is often used to treat Parkinson's disease. The precursor of dopamine can cross the blood-brain barrier and at least partially compensate for the dopamine deficiency in the brain, which leads to symptom relief. A causal treatment is not possible.


.jpg)


.jpg)


.jpg)




.jpg)