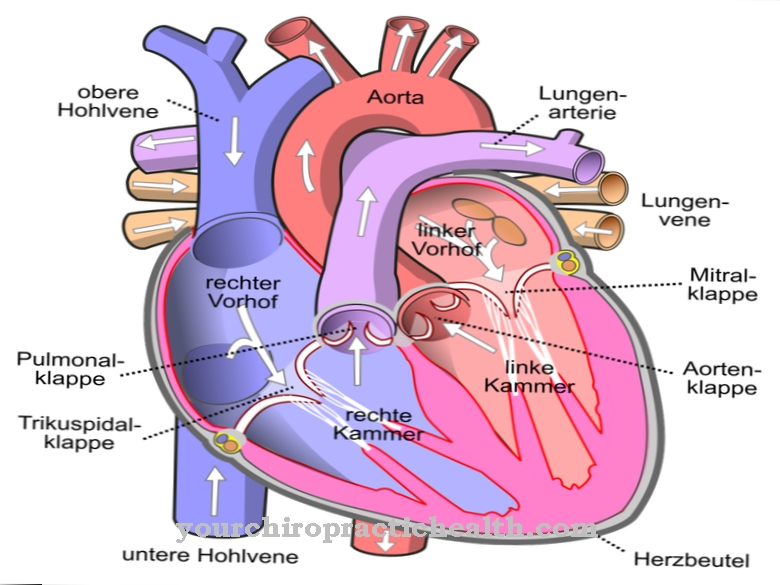
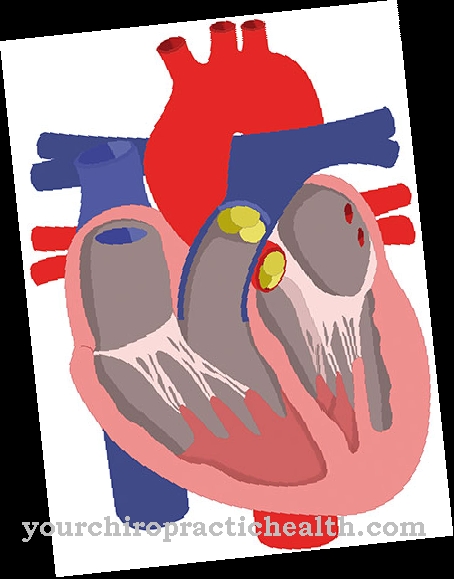
While the heart with its pumping capacity is responsible for maintaining the blood circulation, four heart valves ensure that the blood always flows in the same direction. The two Pocket flaps are located in the initial area of the large arterial outlet vessels of the two heart chambers. The pulmonary valve serves as the outlet valve of the right ventricle to supply the pulmonary circulation and the aortic valve is the outlet valve of the left ventricle to fill the circulatory system.
What is the pocket flap?
A total of four heart valves ensure that the blood in the lungs and in the body always has the same direction. The two heart valves that direct the blood flow from the atria into the chambers are designed as so-called leaflet valves. They serve as exit valves for the atria and as entry valves for the chambers.
Both leaflet valves are closed during the tension and contraction phase (systole), while the two pocket valves, the pulmonary valve (valva trunci pulmonalis) in the right ventricle and the aortic valve (valvae aortae) in the left ventricle open during systole. To prevent blood from flowing back into the chambers from the arterial pressure vessels, the ventricles close during the subsequent relaxation phase (diastole).
By closing the pocket flaps, a residual diastolic pressure is maintained in the arterial vessels. This is the lower blood pressure value. In contrast to the two sail flaps, which differ a little anatomically due to their equipment with 2 or 3 sails, the two pocket flaps are largely identical.
Anatomy & structure
The two pocket flaps are installed in the 5th to 7th week of pregnancy. The three crescent-shaped pockets of each valve develop from the intima, the innermost layer of the arterial outlets in the two heart chambers.
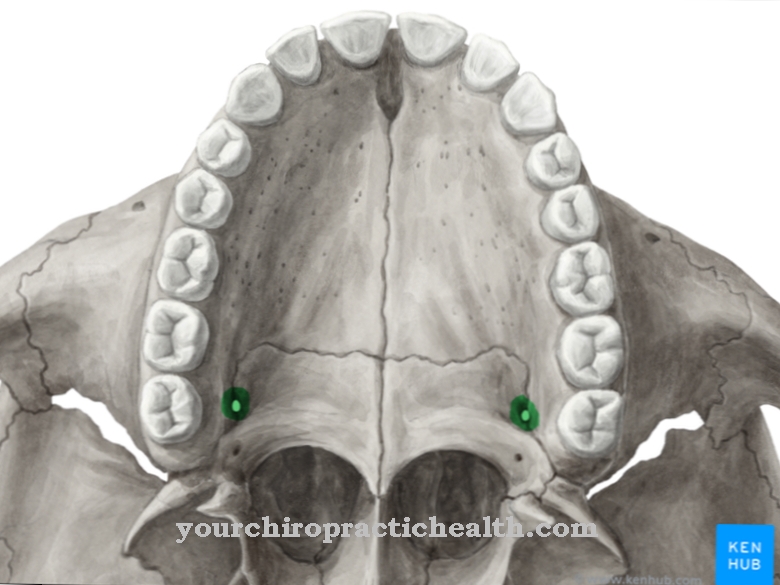
At the end of each pocket there is a small nodule (nodulus valvulae semilunaris) that is embedded in a valve membrane. The nodules serve to support the valve function. The right pocket (valvula semilunaris dextra), the left pocket (valvula semilunaris sinistra) and the anterior pocket (valvula semilunaris anterior) develop in the entrance area of the short arterial pulmonary trunk in the right ventricle, the truncus pulmonalis. The aortic valve, which is located in the entrance area of the aorta in the left ventricle, is also the two right and left crescent-shaped pockets and the pocket facing the ventricular septum (valvula semilunaris septalis).
Since the two arterial branches of the coronary arteries are located directly in the indentation of the left and right pockets of the aortic valve, they are referred to in German as right coronary, left coronary and acoronary pockets (without coronary branching). Both pocket valves are basically the same, but the aortic valve is more powerful than the pulmonary valve due to its higher load.
The aortic valve is occasionally formed from only two pockets, which can be traced back to a genetic anomaly of the valve system, without necessarily resulting in a serious inoperability. The risk that a stenosis, a narrowing of the valve cross-section, results in later years of life is, however, significantly higher than with a normally applied valve.
Function & tasks
The main tasks and functions of the pocket valves are to prevent blood flow back into the ventricles during diastole and to maintain diastolic blood pressure in the arterial vascular systems of the body and pulmonary circulation. Both functions require that the pocket flaps release a sufficiently large cross section during the systolic phase of the chambers to fill the arterial vascular system with the respectively intended amount of blood and that the systolic blood pressure can be set correctly.
If there is a narrowing of the pocket valves, one speaks of a stenosis and, if it is incorrectly closed during the diastolic phase, of an insufficiency. The insufficiency can be divided into different classes depending on the severity. The perfect functionality of the pocket flaps in connection with the perfect functionality of the two leaflet flaps, which separate the atria from the chambers, is one of several prerequisites for normal cardiac output and for ensuring that the heart muscles do not thicken (hypertrophic cardiomyopathy) due to constant excessive demands due to the present Stenoses or insufficiencies.
Diseases
In principle, stenoses or insufficiencies or a combination of both errors can occur in all four heart valves. In the case of stenoses, the heart valves open up an insufficiently large cross-section for blood flow, so that the heart has to produce a higher pumping capacity to compensate.
In the case of heart valve insufficiency, the corresponding heart valve no longer closes correctly, so that in the case of the pocket valves during diastole, blood flows back into the chambers from the aorta or from the trunk of the pulmonary arteries. This is also sufficient reason for the chambers to respond with increased pumping capacity, which in the long term can lead to hypertrophication of the myocardium, as in a stenosis. Stenoses or insufficiencies of the pocket valves can be acquired through illness or exist as congenital heart valve defects from birth and are caused by genetic defects. Aortic valve stenosis is relatively common and accounts for around 43 percent of all heart valve defects in Europe.
The stenosis can be caused by inflammatory processes or the three pockets are calcified. The reasons for the development of aortic valve insufficiency are mostly inflammatory processes, in the course of which there is a partial degradation of the pocket valves or which causes an expansion of the aortic valve ring. Pulmonary valve defects are extremely rare. The most common cause of a stenosis on the pulmonary valve with a corresponding narrowing are genetic factors, which usually have other more or less serious heart defects in their luggage from birth.
Insufficiency of the pulmonary valve is also relatively rare. A leak in the pulmonary valve can gradually set in with pulmonary hypertension or with widening or bulging in one of the pulmonary arteries.




.jpg)


.jpg)





.jpg)
