A Trigeminal neuralgia or Facial neuralgia is the disease or overstimulation of the 5th cranial nerve. The symptoms are severe attacks of pain in the face. Treatment is initially carried out with medication; in severe cases, surgery may be necessary.
What is trigeminal neuralgia?
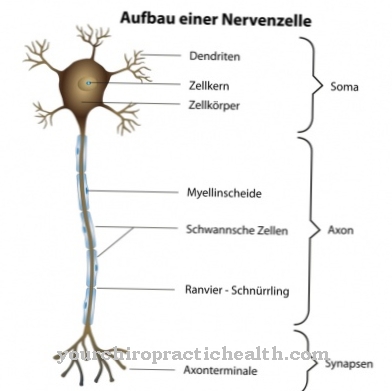
The Trigeminal neuralgia is a disease of the trigeminal nerve. With its three branches (trigeminus = triplet) it innervates the face, the chewing apparatus and the throat and is directly connected to the brain. It belongs to the 12 cranial nerves and is known as the 5th cranial nerve.
Neuralgia is the medical term for nerve pain (neuron = nerve, algia = pain). Trigeminal neuralgia manifests itself in attack-like pain in the cheek, in the upper and lower jaw as well as on the forehead, around the eye or in the frontal sinus.
A distinction is made between symptomatic and classic trigeminal neuralgia. The less common symptomatic form occurs as a side effect to other underlying diseases, often in multiple sclerosis or after a stroke. It often arises on both sides. Classic trigeminal neuralgia is the more common type. It usually only develops on one side and is characterized by symptom-free intervals.
causes
The cause of a Trigeminal neuralgia is damage to, overstimulation or disease of the 5th cranial nerve (trigeminal nerve). In classic trigeminal neuralgia, the trigger is usually increased pressure on the nerve.
This is caused by thickened blood vessels. When arteries become calcified, their elasticity decreases and they become thick and immobile. If such a thickened artery is close to the nerve, it creates pressure and causes irritation or damage to the nerve.
In the rarer symptomatic trigeminal neuralgia, the cause is another disease. In multiple sclerosis, the nerves become inflamed and trigger trigeminal neuralgia; in the case of a stroke, a circulatory disorder in the brain can cause the neuralgia.
Symptoms, ailments & signs
The main symptom of trigeminal neuralgia is a strong unilateral pain in the face that shoots in suddenly and with a pull. It almost feels like a lightning-like surge of electricity that subsides again after a short time. Sometimes the pain is also perceived as burning or stabbing. Depending on which branch of the trigeminal nerve is affected, the symptoms lie in the corresponding area of the face.
The second and third branches are most often affected. This leads to pain in the cheeks, cheekbones and chin, nose or upper and lower jaw. Teeth can also hurt. On the other hand, complaints on the forehead, where the first nerve branch runs, are rare. The pain attacks can be triggered by touching the skin, by a draft of air, by brushing your teeth, by moving the jaw while speaking or chewing or by swallowing.
However, they can also flare up suddenly and without prior stimulus. Sometimes the shooting pain is accompanied by twitching of the facial muscles. The trigeminal nerve is one of the thickest nerves in the body, so the pain it causes is almost unbearable.
For fear of a pain attack, some patients refrain from ingesting food and fluids. This can cause weight loss and dehydration. Since the symptoms are extremely stressful, the disease can lead to depression.
Diagnosis & course
The complaints in one Trigeminal neuralgia are mainly expressed in sudden, severe pain in the face that lasts only a few seconds and then subsides again. They feel like power surges and can repeat themselves at several short intervals and then go away for a period of time.
Often these pain attacks are triggered by touching the face or by moving the jaw. It can happen while chewing or swallowing, brushing your teeth, or speaking. Sometimes the attacks are also triggered by a draft. The pain of trigeminal neuralgia is one of the most severe pains there is. Those affected often avoid eating or speaking as this will trigger the pain attacks.
In order to be able to make a clear diagnosis of trigeminal neuralgia, the doctor must first ask about the patient's medical history and examine him neurologically. A dental, orthopedic and ENT examination can rule out other diseases with similar pain. Magnetic resonance imaging (MRI) can be used to detect previous strokes, tumors, or inflammations that may be the trigger for trigeminal neuralgia.
Complications
The extremely painful trigeminal neuralgia can lead to various complications. These are mostly classified as postoperative complications. Due to the severe pain that occurs in attacks, those affected with trigeminal neuralgia can suffer from pain-related depression.
Apart from the medical treatment goal of achieving permanent pain relief, psychotherapeutic interventions are sometimes necessary. If the pain attacks of trigeminal neuralgia cannot be relieved with medication - or if these side effects are too severe - surgical methods are common. The previous transection of the trigeminal nerve usually led to partial facial paralysis.
Since this surgical method often caused more pain than before, this method of treatment has been abandoned. But even the surgical methods used today are not without risk. In the case of symptomatic trigeminal neuralgia, the potentially possible complications can be shaped by the underlying disease.
It can be cancer or multiple sclerosis. Corresponding complications such as metastasis, paralysis or blindness are conceivable. After operations on the ganglion gasseri, tenderness, sensory disturbances or even greater pain may occur. However, these are mostly permanent pain.
With microvascular decompression, there is an increased risk of anesthesia and a higher risk of complications. The procedure occasionally results in unilateral hearing loss, bleeding, or cerebellar swelling. When the irritated trigeminal nerve is irradiated with a linear accelerator, there are comparatively fewer complications. The success rate is significantly lower.
When should you go to the doctor?
Since trigeminal neuralgia is accompanied by massive facial pain, the person concerned should see a doctor quickly. This must determine whether there was a specific trigger or whether it is an idiopathic trigeminal neuralgia.
In the symptomatic variant of trigeminal neuralgia, the underlying problem must be identified as soon as possible. Only then can targeted treatment begin. In the course of this, the massive facial pain can also disappear.
A quick visit to the doctor is also advisable because the severe pain symptoms in the facial area can conceal a late complication of shingles, a tumor or multiple sclerosis. Stroke symptoms or borreliosis have also already been identified as triggers for symptomatic trigeminal neuralgia. Tumors are rarely the cause of trigeminal neuralgia. If they are, however, the tumors can be both benign and metastatic extensions of an undiscovered tumor.
In sum, the possible triggers are serious enough not to endure trigeminal neuralgia for months on self-prescribed pain medication. That being said, the pain in trigeminal neuralgia is often massive. As a result, going to the doctor often happens on its own.
Treatment & Therapy
The Trigeminal neuralgia is initially treated with pain relievers. The usual pharmacy-only drugs are ineffective here, however, as the pain is extremely strong. If a large number of pain attacks occur one after the other in a short period of time, intravenous treatment is given with a high-dose anti-epileptic.
For this therapy in the case of an acute attack, inpatient admission to a hospital is necessary. To prevent the pain attacks, anti-epileptic drugs are given as tablets in lower doses, but permanently. If there are other underlying diseases, these must be treated primarily, as they are the triggers for trigeminal neuralgia.
If the drug treatment does not improve, an operation is possible. The cranial bone is opened in a surgical procedure in order to free the nerve from constricting vessels. Radiosurgical therapy is another treatment option that does not require surgical opening of the skull. The nerve is treated with rays through the bone.
A third option for treating trigeminal neuralgia is percutaneous (through the skin) thermoagulation, in which a probe is pushed to nerve cells of the trigeminal nerve under short anesthesia and the pain fibers of the nerve are destroyed there with heat.
You can find your medication here
➔ Medicines for painprevention
Against a Trigeminal neuralgia cannot be prevented. However, a balanced diet and a healthy lifestyle can prevent hardening of the arteries, which is often the cause of trigeminal neuralgia.
Aftercare
If trigeminal neuralgia is treated with surgery, follow-up care is required. In most cases, the symptoms improve immediately after the operation. Computed tomography (CT) usually takes place on the day of the operation as a check-up. This enables the doctor to diagnose possible air pockets or secondary bleeding.
The patient spends the first five to six days after the operation in the hospital. After that, he is usually released. Outpatient care is usually sufficient to remove sutures or staples. As a rule, there are no restrictions to fear after the hospital stay. Most patients no longer suffer from health problems after discharge.
The pain relievers that the patient has taken so far should be reduced step by step in consultation with a neurologist or pain therapist. The therapist provides supportive care. In rare cases, symptoms in the scar area, headache, fever or the discharge of clear liquid from the nose occur after the operation. In this case, the person concerned must see a neurosurgeon. Rehabilitation does not need to be started.
It usually takes about three to four weeks before the patient is allowed to exercise again. During this period, stays in the sauna or the blazing sun should also be avoided, as otherwise dizziness or headaches may occur.
You can do that yourself
The possible self-help measures for trigeminal neuralgia are limited. They extend to support medical treatment and are general in nature.
Avoiding stress and eating a balanced diet contribute to well-being. Some patients rely on autogenic training or other relaxation techniques. Others have stepped down professionally and have integrated rituals that allow time off into their day. Regular exercise is also an important factor in alleviating a new pain attack. The consumption of nicotine and alcohol should be completely stopped. These measures do not necessarily prevent all complaints. However, due to increased well-being, they do not make the symptoms appear so troublesome.
The everyday life of those affected is severely impaired because the attacks can recur. Some patients suffer from chronic anxiety. This often results in a withdrawn life without undertakings. As a result, depression often sets in. Escaping this state of affairs can be difficult. A strong environment and social contacts promise a positive way of dealing with trigeminal neuralgia. Contact with like-minded people sometimes also helps. In self-help groups, experiences and tips on coping with everyday life can be exchanged.
.jpg)

.jpg)















.jpg)