The accessory nerve is a motor nerve known as eleventh cranial nerve is known. It has two different branches and motor innervates the sternocleidomastoid and trapezius muscles. Damage to the nerve can lead to head-turning or trapezius paralysis.
What is the accessory nerve?
In the human body, the nervous system consists of motor, sensory and mixed nerves. Sensitive nerves are responsible for the transport of stimulus perception in the form of excitation. Motor nerves are responsible for active reactions to the environment in the form of reactive movements and voluntary movements. Mixed nerves are nerves with parts of both sensory and motor fibers.
The accessory nerve or eleventh cranial nerve is a motor nerve that consists of two different branches in the sense of rami. The internal branch has its origin in the brain stem and the external branch arises from the spinal cord. Cranial nerves are all those nerves that arise directly from specialized nerve cell clusters or cranial nerve nuclei in the area of the brain.
Like a portion of the accessory nerve, most cranial nerves arise directly from the brain stem. Although another part of the accessory nerve arises from the spinal cord, it is caught under the cranial nerves.
The eleventh cranial nerve was first described by Thomas Willis and, due to its two different origins, includes a spinal cord and a skull root in its anatomy. The spinal radix or root of the spinal cord of the accessory nerve comes from the upper neck segments on the spinal cord. The cranial radix or root of the skull originates below the vagus nerve, where it emerges from a groove called the posterolateral sulcus within the medulla oblongata.
Anatomy & structure
The radix spinalis emerges from the spinal cord in the lateral area. The fibers of the root originate in a collection of motor neurons, in the so-called nucleus motorius nervi accessorii or nucleus principalis nervi accessorii. The individual nerve fibers in the subarachnoid space rise along the spinal cord. They pass through the foramen magnum in the area of the posterior fossa. The cranial root receives branchio-motor fibers from the so-called nucleus ambiguus, which with its fibers is involved in several cranial nerves.
The fibers of the external and internal ramus join within the skull and exit through the jugular foramen from the skull, where they separate again. The internal ramus runs intracranially to the side of the medulla oblongata and sends fibers to the jugular ganglion.
After being separated outside the skull, the rami join the vagus nerve and the branches to the pharynx and larynx. The external ramus enters the lateral funiculus of the spinal cord and extends cranially to leave the spinal cord again in the area of the posterior lateral sulcus and emerge as an independent nerve cord into the foramen magnum and out again.
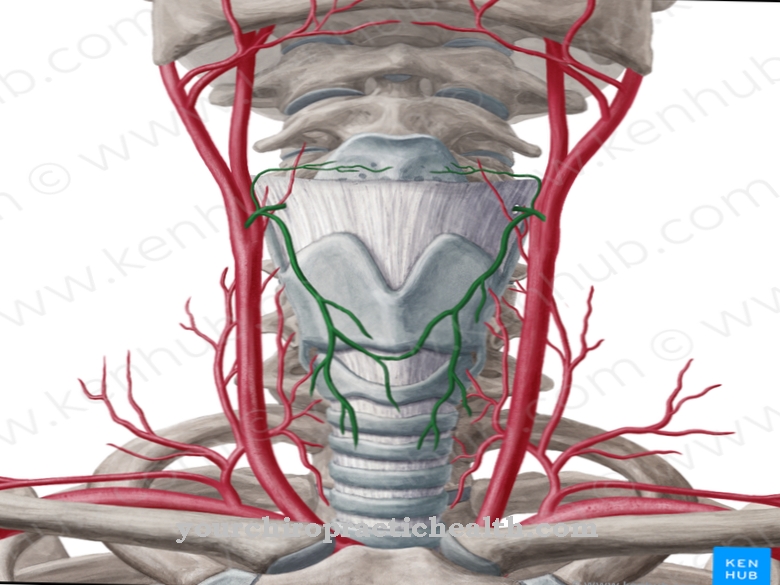
After exiting the skull, the external branch runs caudally and runs ventrally or dorsally along the internal jugular vein. The ramus thus reaches the sternocleidomastoid muscle and the trapezius muscle, where it picks up fibers from the cervical plexus and forms a network.
Function & tasks
The accessory nerve is a motor nerve. As such, it is responsible for the motor connection of muscles to the central nervous system. Motor nerves transmit commands from the central nervous system to the muscles efferent, causing them to contract or relax. The radix spinalis of the accessory nerve supplies the sternocleidomastoid muscle and the trapezius muscle with motor fibers in the form of the external ramus and is therefore involved in the contraction of these two muscles.
The trapezius lies on either side of the upper spine and runs from the occiput to the lower thoracic vertebrae. Laterally it extends to the shoulder blade. The trapezius muscle is responsible for various movements. He is responsible for raising the arms above the horizontal and is solely involved in rotating the shoulder blades upwards and towards the center.
The sternocleidomastoid muscle is a ventral neck muscle known as the large head turner. It causes the head to tilt sideways towards the shoulder and is involved in the slight extension of the head backwards. Both muscles, which are motor-innervated by the accessory nerve, are presumably sensitively innervated via the rami musculares of the cervical plexus.
You can find your medication here
➔ Medicines for paresthesia and circulatory disordersDiseases
The condition of the accessory nerve is clinically checked by turning the head against resistance. When the nerve is paralyzed, the affected shoulder hangs. This phenomenon corresponds to trapezius paralysis, which prevents the arm from lifting above the horizontal.
Proximal nerve damage is associated with tumors of the skull base. Partial paralysis is often preceded by removal or a biopsy of the cervical lymph nodes within the lateral triangle of the neck, as is done in cases of suspected tuberculosis and other lymphomas.
More rarely, lesions of the accessory nerve are caused by whiplash injuries. Just as rarely, abnormalities of the craniocervical junction or skull base fractures are the cause. In patients undergoing radiation therapy, lesions of the nerve could correspond to radiation damage. Distal nerve damage to the accessory nerve is usually preceded by surgical removal or other disease of the cervical lymph nodes.
In addition, syringomyelia and poliomyelitis can damage the accessory nerve in the area of the anterior horn of the spinal cord and thus cause functional impairment of the muscles it innervates. Syringomyelia are usually associated with CSF outflow disorders. Poliomyelitis is polio that is caused by a viral trigger.







.jpg)

.jpg)
.jpg)











.jpg)